
42 Attorneys General Demand Surgeon General Warnings On Social Media In a move that's undoubtedly going to be used to...
Read More

Send This Article To People Who Say “Ivermectin Doesn’t Work For Covid-19”
Authored by David Gortler via the Brownstone Institute,
If you hear your pharmacist, physician, or academic dean parrot the malignant regurgitated trope of “Ivermectin doesn’t work for Covid” or that there is “no evidence” or “no data” to support ivermectin’s use in Covid-19, send them this meta-analysis summary and annotated bibliography of over 100 studies.
{kind=link}
I never really latched on to the idea of social media, which is why I never signed up for it. In addition to pathological social factors, I think it is an especially absurd format for serious scientists to initiate a debate on the intricacies and complexities of medical research, clinical pharmacology, or patient care.
I did not have a Twitter/X account but very recently created one after I was contacted by colleagues alerting me to posts from Dr. Peter Hotez criticizing my recent testimony before the House Select Subcommittee on the Coronavirus Pandemic held by Dr. Brad Wenstrup (R-OH). Dr. Hotez is a pediatrician and tropical medicine Dean at Baylor in Houston, Texas. About six weeks later, Dr. Hotez responded to my testimony on Twitter/X:
“To the countries, physicians, & pharmacists who prescribed ivermectin or hydroxychloroquine…you were right.” – Dr. Gortler
Never forget the so-called experts and shills who gaslit Americans about COVID treatments and the vaccine. pic.twitter.com/UJInVqdSdb
— Heritage Foundation (@Heritage) May 8, 2024
I attempted to rebut Dr. Hotez’s statement by setting up a Twitter/X account only to find out that I couldn’t! Little did I know that the only way to comment on Dr. Hotez’s public Twitter/X page was to be granted permission by him to do so!! And here I thought the idea of Twitter was to foster discourse; not stifle it.
{kind=link}
It certainly appears that dissenting scientific opinions are not welcome on Dr. Hotez’s Twitter/X page.
Dr. Hotez’s critique of my testimony was not an invitation to discuss the merits or shortcomings of ivermectin therapy; it was a figurative “drive-by shooting” stating that my sworn Congressional testimony was:
“dangerous anti-science disinformation, pure and simple” and that
“Ivermectin does nothing to help people with Covid” and
“Ivermectin doesn’t work for Covid”
The second (in a list of around a dozen short, subsequent tweets by Dr. Hotez) was a pitch for his book.
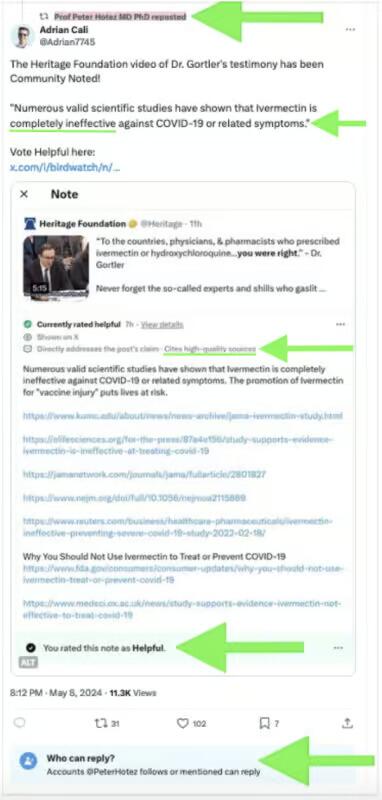
Dr. Hotez then “upvoted” and reposted a note from one of his selected followers who appears to be a Twitter moderator of some sort. This individual had gleefully declared that my testimony had been “community-noted” adding that “Numerous valid scientific studies have shown that ivermectin is completely ineffective” (emphasis added) and “the promotion of Ivermectin for vaccine injury puts lives at risk.” The latter statement was a sleight of hand, as I had never opined on the use of ivermectin for “vaccine injury” at any time during my testimony or in any of my previous writings.
Twitter’s community notes are intended to give context to posts with debatable data, with this one, purporting to “debunk” my testimony, containing seven (7) reference links. Two of the links were duplicates, referring to the exact same data (numbers 1 and 3 and numbers 2 and 7). They referred to JAMA or NEJM studies which in turn have been criticized by academics as having very significant scientific and clinical practice shortcomings. Although the note additionally specified that “the promotion of ivermectin for ‘vaccine injury’ puts lives at risk,” none of those links determined that the use of ivermectin poses a safety “risk.” When prescribed correctly, ivermectin has not only been determined to be safe, but it has historically proven itself to be “astonishingly safe.”
The second-to-last “community note” link was a non-working link to an FDA website. It didn’t work because the FDA had agreed to delete it over a month earlier as part of a legal settlement for improperly denigrating ivermectin use. Didn’t the Twitter/X “community note” staffers bother to click on the links to make sure they worked before permitting them to be posted as references? Eventually, other individuals noticed the palpable shortcomings of the “community note” as well because it was quickly removed despite stating that it “Cites high-quality sources.”
A picture of the original “community note” with added arrows highlighting specific areas is shown below:
{kind=link}
Of course, neither myself nor anyone else could contradict those claims because we were all blocked from posting by Dr. Hotez. It appears that he would rather make an incorrect assertion, then stick his fingers into his ears after he was finished saying what he had to, running away from any potential discussion, while his “approved” posters swarm to up-vote him – but all while potential counterarguments can’t be posted.
With no outside dissent allowed, does that mean Dr. Hotez “won” the debate?
It turns out my foray into Twitter was misguided and a waste of time. My Twitter/X account is now history. While it works great for a myriad of different matters, it is obviously an absurd place for a serious person to attempt to discuss or debate the intricacies of medical science or patient care. At this point, I have no intention of returning.
Ignoring and Censoring Data in History: Copernicus and Galileo
Consensus is very important to some, but unfortunately, it isn’t related to science. Science doesn’t care about consensus. In fact, many of the biggest scientific advancements were the result of questioning an established consensus. Generating a consensus for a new, controversial topic can be particularly dangerous. When people agree they tend to support each other, but a danger exists that they forget that they are reaffirming a potentially incorrect or polarized belief because their decision-making is biased and/or occurring in a vacuum.
In almost exclusively permitting harmonically positive feedback for himself, Dr. Hotez has failed to consider that it was artificially cultivated with essentially no meaningful dissent allowed to take place. In addition to being anti-free speech, it’s a terrible example for a scientist to set, particularly for someone in the position of a professor educating future scientists. The best scientists are the ones who are willing to listen to the opinions of other intellectuals and consider their arguments.
History shows us that ignoring scientific evidence and quashing dissent isn’t good for technical advancement; something that a professor who also labels himself a “science warrior” on his own homepage probably ought to already know.
A textbook example of “anti-science” was when Copernicus and Galileo tried to advance theories that the earth rotated around the sun (as opposed to the heliocentric narrative of the earth being the center of the universe, around which all celestial objects rotated). Copernicus and Galileo were ignored and their writings were banned. Both were tried by a panel of their peers, found guilty, removed from their didactic pulpits, arrested and imprisoned. Galileo was eventually permitted to live out his remaining years, exiled under “house arrest” away on a farm. But even then, at least both Copernicus and Galileo were given opportunities to argue and present their evidence…unlike Dr. Hotez’s blockaded Twitter account.
Medicine is Rarely “Black or White”
Despite decades of advancement, clinical science is seldom black or white. Only very rarely are there declarations “never” or “nothing” or “completely.” Still, Dr. Hotez routinely makes polarizing, binary black-or-white, right-or-wrong assertions from his “members-only” perch on Twitter/X, neglecting or ignoring data – and it’s not just for Covid treatments.
A great deal of medical and pharmacology research deals with levels of uncertainty, something which I regularly taught my students and hoped that most medical scientists already knew and understood. Declarations otherwise would be irresponsible emerging from any medical scientist, let alone one with Dr. Hotez’s credentials.
Dr. Hotez’s unambiguous declarations that: ivermectin is “completely ineffective” and ivermectin’s use represents “anti-science disinformation pure and simple” are simply not reflected in both the review of many clinical trials and larger statistical analyses of published literature. In fact, there is data that sharply and directly contradict Dr. Hotez’s statement that “Ivermectin does nothing to help people with Covid.”
It is my belief that the continued accumulation of positive findings for ivermectin will continue and show an even greater positive effect for Covid pre-exposure prophylaxis, early exposure, and early treatment modalities. Like a good scientist, I am open-minded and am willing to hear out intellectual, alternative thoughts from my detractors. That being said, I have a considerable amount of data backing up my opinion.
Response to Dr. Hotez’s Assertion: “Ivermectin Does Nothing to Help People with Covid”
Since I am not permitted to respond on Twitter/X, (in addition to the fact that it is not an appropriate platform to discuss the complex details of clinical trial data) I’m responding in the form of a review, analysis, and lengthy, annotated bibliography.
Academics should encourage the discussion of controversial topics. In composing an argument, one needs to present all available data – not exclusively preferred findings from selected “big name” domestic medical journals (which by the way are often heavily financed with expensive advertisements from Big Pharma) – but legitimate clinical and scientific data from all sources.
First, publications in “big name” journals like the NEJM and JAMA are not holy scripture beyond critique. Also, there is legitimate research being conducted in non-US countries and/or published in smaller journals worthy of consideration. On top of that, those who spend their lives in medical research will tell you that non-NEJM and non-JAMA, non-“big name” smaller, observational, and/or real-world study data are not only very worthy of consideration, but that those study designs and results can often be even more reflective of a drug’s utility and safety.
Cochrane’s Ivermectin Review is Incomplete
Cochrane’s March 2024 review of ivermectin has been cited as a source of data for ivermectin being ineffective. However, Cochrane only considered 11 Randomized Controlled Trials (RCTs) covering 3,409 participants. For ivermectin, there are 50 RCTs covering 17,243 participants which when analyzed in combination, show very strong evidence for efficacy in Covid-19. The fact that Cochrane selectively excluded a large amount of study data, while simultaneously including low-quality data with high conflict of interest and highly biased study designs, is more than a little perplexing. Of note, Cochrane also didn’t combine all of the evidence from the studies it did choose to include; data was split into very small sets by outcome and patient status, with no method used to combine all of the evidence from independent studies.
It seems to me that Cochrane isn’t what it used to be, and I for one am very disappointed.
Data Analysis
The proper application and weighting of data and its random effects meta-analysis across all studies can provide a complete picture of an effect. It includes all data, including too-low-dose, too-short-duration, less effective late- versus early-treatments, wrongly used fasting dosing (ivermectin is substantially better absorbed with high-fat foods [2.5x greater] according to the Merck package insert).
To date, there exists a list of 103 manuscripts written which studied ivermectin. Those data also include 15 medRxiv and/or preprint articles, (for journals that refuse to defy Big Pharma narratives and/or potentially those that the White House has ordered censoring) and all studies that showed ivermectin’s effectiveness with some certitude, but not at the level of p≤0.05. On a side note: inclusion versus exclusion of the medRxiv/preprint articles does not alter the overall positive ivermectin treatment effects.
These clinical findings are in addition to the highly plausible molecular biology and pharmacology mechanisms of how ivermectin is potentially effective for preventing the entry of some viruses into cells. For purposes of keeping the length of this document manageable, the pharmacologic mechanism of action will not be discussed here.
A Value of p ≤0.05 is Important, but it Isn’t Everything
Studies with p-values higher than 0.05 still provide evidence – just evidence with a lower than 95% confidence. Alone, those studies may not provide statistical confidence by themselves against the null hypothesis. However, they may contribute to a meta-analysis, in which they are weighted appropriately. In an analysis, they may actually result in strong statistical evidence and greater confidence from the combination of data from multiple independent scientific teams. Smaller studies and real-world observational studies should not always be dismissed as non-evidential; even case reports and case series have historically played an important role in biomedical research and the assessment of drug safety. In fact, those sources of data were part of what I routinely considered in approving new drugs and labeling updates during my years at the FDA as a drug safety expert.
RCTs are conceptually preferred if properly designed and carefully conducted, but the Covid era exposed severe biases in such trials: including but not limited to treatment delays (as Covid-19 along with any antiviral treatment must begin promptly) protocols that were designed to fail, mid-study changes, biased analysis and presentation, and lack of transparency in data and suspiciously timed publication releases. Each study should be evaluated for potential biases and/or confoundings on its own merit, whether randomized or observational, large or small.
Major RCTs allegedly producing Big Pharma-coined-term of “Evidence-Based Medicine™” published in “big journals” can appear very compelling, especially because they are what the lay press tends to cite most commonly, but clinicians should know that it is important to examine the methodology used beyond the high-level summary overviews and to also look at additional sources of data.
Another problem with RCTs is that, unlike real-world and observational studies, not just anyone can conduct large RCTs. Barriers include them often being significantly more expensive, time-consuming and requiring a dedicated, highly skilled support staff. Those sorts of requirements prohibit entry by less-well-funded clinicians who have smaller practices/facilities or those that have employment requirements which have a focus on direct care responsibilities as opposed to clinical research. While federal grants are available, they are highly competitive and tend to be limited to particularly listed topics which in turn end up being awarded to a limited number of major centers with those aforementioned resources.
Those major centers and/or their employees can be connected in one way or another to Big Pharma funding. For highly profitable Covid-19 drug trials, it could directly or indirectly create a conflict or incentive to show a lack of effectiveness or safety for inexpensive generic products, and in turn show efficacy for novel, expensive patented commercial products. This scenario not only applies to Covid-19 treatments such as ivermectin, it applies to a fair amount of all investigational medicine research.
In fact, a multitude of smaller, less expensive non-RCT observational/real-world-use studies across many facilities can make a stronger case by noting that dependence on any individual trial is subject to potential confounding, errors, bias, and even fraud. Therefore, the combined evidence from multiple, well-designed and conducted smaller, real-world, case reports, case series, and/or observational trials from an array of smaller facilities, combined via meta-analyses can sometimes be a stronger indicator than that of just one or a few biased large trials.
A diagram adapted from a Nature publication (below) illustrates a scenario in which 4 (four) smaller studies that individually may not have delivered statistical significance (ie, have a p>0.05) but when considered in combination, may provide strong evidence with a statistical significance via meta-analysis:
{kind=link}
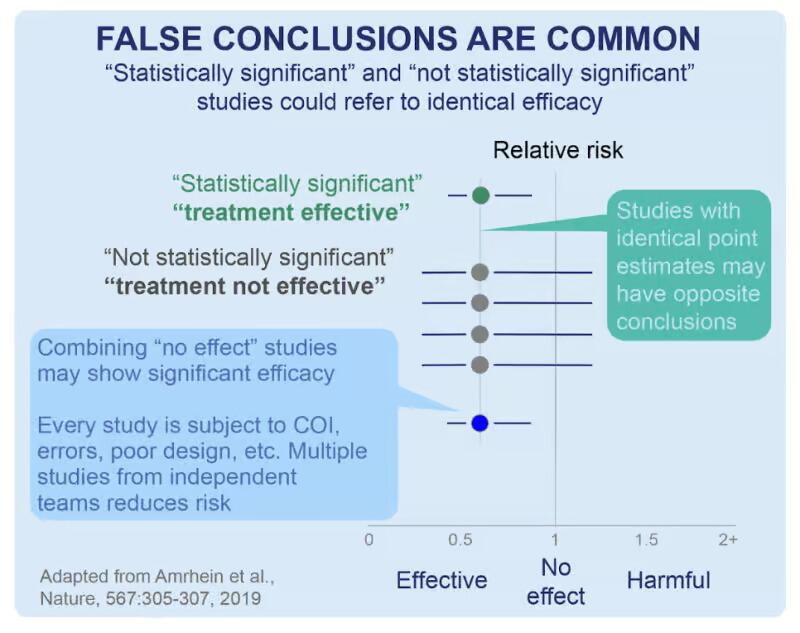{kind=link}
Separately, that same publication additionally underscores how important it is for scientists and clinicians to not mistakenly assume that “non-significance” (ie, a higher deviation from p≤0.05) translates to “no effect.” Statistical significance is just a numerical estimate of the confidence of a result. The idea that a small p-value implies that the estimate is credible/true/valid /the-only-thing-that-matters is a misconception. A small p-value of an RCT (for instance) says nothing about the quality of the estimate.
In the matter at hand, and in summation, a random-effects meta-analysis shows a clinically beneficial effect of ivermectin with a certainty of p<0.00000000001 (that is, one in one sextillion) over all 103 ivermectin studies for Covid-19, and also for RCTs and for specific outcomes like mortality hospitalization and recovery cases which all show p<0.0001.
Timing is Everything…(When it Comes to Initiating Antiviral Treatment)
The use of the word “early” in the “c19early.com” website is an important annotation. It reminds us of how critical timing is when it comes to any antiviral/antimicrobial drug administration. Ivermectin as an antiviral works best when administered early upon symptom(s) (or for prophylaxis/pre-exposure). That is the same when it comes to any antiviral pharmacology treatments, including for cold sores, genital herpes, influenza, or HIV/AIDS for instance.
Delayed administration could still have a clinical benefit, but less so, depending on how late and individual factors that include viral replication, infective loading dose, and viral variant/mutation, besides numerous demographic, immunologic, plus other factors. That is a fundamental concept that anyone in the field of pharmacy or medicine should have learned early in their schooling, yet it seems to have been omitted in about half of the 103 studies done on ivermectin which employed delayed or late treatment.
In addition to the delay in ivermectin dosing was the delay in releasing study findings. The worst example might be PRINCIPLE RCT results which were delayed over 800 days from the expected release of findings. PRINCIPLE (bibliography and explanation in reference number 88 below) was biased against showing efficacy per the design, operation, analysis, and reporting, and including very late ivermectin administration, yet still ended up showing a positive effect of ivermectin. During the delay in releasing data, novel, expensive, likely less efficacious “rebounding” Big Pharma treatments like molnupiravir and Paxlovid were developed, (and tested against placebo instead of treatments like ivermectin) reviewed, authorized, and White House-endorsed. Paxlovid ($1,400 per treatment course) and molnupiravir ($700 per course) were each around ten times more expensive than ivermectin (<$100 per course). Paxlovid purchased by the White House cost American taxpayers over $10 billion.
For perspective: the greater than $9 billion savings from the use of ivermectin alone could have instead bought about 36,000 $250,000 Lamborghini Huracans, or alternatively for those of us who must work for a living, about 300,000 $30,000 Toyota Camry SEs (the most popular model).
For Covid-19, There is More to the Data than Just Press/Abstract “Topline Results”
To fully address transparency, I am including a full list of ivermectin studies completed to date, with the plurality of positive and negative findings in the form of an annotated bibliography at the end of this article to allow readers to see the sources of the research. Each of the 103 references includes a brief summary and a link to a longer analysis at c19early.
Along with the bibliography, I am also including two summary plots of the ivermectin data from c19early on overall benefit, and relative benefits from prophylaxis, early, and late treatments.
Click here to see annotated bibliography.
Tyler Durden
Tue, 06/11/2024 – 23:40